|
Autism Epigenetics News Updates from the Escher Fund for Autism, July 2015
______________________________________________ A Father Prenatally Exposed to Synthetic Hormones, a Son with Idiopathic Severe Mental Illness and Autism: Is Germline Epimutation to Blame? [See our blog for the story. The author is the father of a nine year-old boy with multiple mental and developmental disabilities. He lives in California.] Related stories: • Chrissy's prenatal drug exposure story: A Glut of Abnormal Neurodevelopment in One Family — Did Grandma's 1960s Pregnancy Drugs Cause Germline Errors? • Joan's prenatal drug exposure story: A Mother of Three Children with Autism Speaks Out About Her Prenatal Exposure to Synthetic Steroid Hormone Drugs • Jill's prenatal drug exposure story: A Generation of Drugged DNA? ______________________________________________ $25k RFP due June 30, 2015: Parental Germline Exposures in the Histories of Autism Multiplex Families Autism is highly heritable without being "genetic" in the classic sense, and its rates are skyrocketing, up 28-fold in California's DDS system since 1987. We hypothesize that a subset of ASDs arise from induced epigenomic and/or genomic disruptions of parental germline during the vulnerable early phase of fetal germline synthesis. This new RFP asks investigators to look at F2 ASD multiplex families to probe this idea, with an emphasis on ascertainment of F1 in utero pharmaceutical and other acute exposures, such as maternal smoking, in the 1950s, 60s, and 70s. RFP details can be found at: germlineexposures.org/grants. ______________________________________________ New Papers in Cell Suggest Distinctive Epigenetic Treatment for Neurodevelopment Genes on Human Germline It appears some areas of our DNA methylome are not entirely erased during gametogenesis. New research indicates that about five per cent of our genetic code carries molecular traces of past exposures, and may by leaving a devastating legacy for children and grandchildren. Professor Azim Surani, from the Wellcome Trust/Cancer Research UK Gurdon Institute at the University of Cambridge, said: “The information needs to be reset in every generation before further information is added to regulate development of a newly fertilised egg. It’s like erasing a computer disk before you add new data." But 5% of the genome are ‘escapee’ regions which contain some genes that are particularly active in neuronal cells, which may serve important functions during development. Walfred Tang, a PhD student who is the first author on the study, said: “Our study has given us a good resource of potential candidates of regions of the genome where information is passed down not just to the next generation but potentially to future generations, too.” See the paper in Cell: A unique gene regulatory network resets the human germline epigenome for development Also published in Cell: DNA Demethylation Dynamics in the Human Prenatal Germline The Transcriptome and DNA Methylome Landscapes of Human Primordial Germ Cells ______________________________________________ Worth a Watch: Epigenetics and Intergenerational Inheritance Professor Marcus Pembrey (co-recipient of our recent grant on fetal germline effects of maternal smoking, with Professor Jean Golding) is featured in this new YouTube video, featuring Dr. Elizabeth Radford as well. https://www.youtube.com/watch?v=_3lXZ_ZgSmI ______________________________________________ The Germline Disruption Hypothesis of Autism, in an Infographic http://www.germlineexposures.org/blog/the-germline-disruption-hypothesis-of-autism-in-an-infographic ______________________________________________ Reminder: Mini-grants Available, No Deadline Mini-grants in the $250-$5,000 range are available on a rolling basis to support meetings, papers, research, or other work related to investigations of the induced germline disruption hypothesis of autism. Simply email us with your inquiry. ______________________________________________ The Escher Fund for Autism supports projects that investigate the role of de novo germline perturbation in the etiology of autism and related disorders. Visit GermlineExposures.org for: • Expert Q&As • Germline epigenetics in the news • Germline development and reprogramming backgrounder • Blog
0 Comments
 [The author is the father of a nine year-old boy with multiple mental and developmental disabilities. He lives in California.] Our son, Jacob (not his real name), is nine years old. He has been diagnosed with a range of mental health and developmental disorders, including autism spectrum disorder, oppositional defiant disorder, mood disorder, anxiety disorder, and most tragically, childhood onset schizophrenia. In spite of multiple medication trials and behavioral and other therapies over many years, Jacob remains violent toward caregivers on a daily basis and less frequently toward peers. In addition, Jacob is chronically internally preoccupied and disconnected from reality, intermittently distressed by paranoia, delusions and the voices only he hears, and his thinking and speech have become so garbled that he is incoherent the vast majority of the time. In a meaningful sense, we have lost and continue to lose gradually the child we once thought we had.
Behind the diagnostic labels, the severity of his abnormal brain development and the impairments in his functioning are obvious. His violent behaviors have become so frequent and dangerous he can no longer live at home. No specialized school or residential treatment center in California—facilities designed to handle children with disabilities like these—would serve him, so we had to send Jacob to a placement 3,000 miles away, after he spent the majority of the last 16 months in hospital and partial hospital settings. While my wife and I each have some very distant relatives with mental illness or autism, none of our 11 nieces and nephews nor any other close relatives have anything like the mental health or developmental challenges that Jacob does. Furthermore, Jacob's disorders are considered "idiopathic" in the sense that clinicians cannot find— despite extensive testing—any prenatal or genetic causes for this most unexpected, traumatic, and truly horrifying outcome in our son. A few years ago, at the prompting of our friend Jill Escher, I asked my mother if I had been exposed in the womb to any fertility or anti-miscarriage treatments. I thought it was a strange question, but Jill had two children with idiopathic autism, and she explained she had just discovered that she had been exposed in utero to synthetic steroid hormone drugs via injections given to her mother at a popular Los Angeles fertility clinic. In Jill's case, her mother had two prior miscarriages and the practitioners of the time felt that supplementing a pregnancy with synthetic hormone cocktail could improve the gestational environment. Jill thought those old drugs could have disrupted the molecular programming of her eggs. So I asked my mother, and the answer, to my surprise, was yes. I was born in 1969 in New York City, and while pregnant with me my mom received treatments at the New York Fertility Institute, but did not recall the names of the drugs used. They treated her with hormones because she had had a D&C due to endometriosis. Though she could not locate those medical records, she said, "I remember taking some injections during the first few months of pregnancy so as not to miscarry." Whether my prenatal exposures to some form of anti-miscarriage hormone protocol of the 1960s affected the development of my gametes, I cannot say for certain. But it's a hypothesis that maps to the emerging research demonstrating adverse fetal germline effects of endocrine-disrupting drugs, and the revelation that the genes most likely to retain epimutations during reprogramming are those involved with neurodevelopment. I hope the tragedy of our son, and that of Jill's autistic children, too, will help prompt more researchers to tackle the germline disruption hypothesis. These "genetic-ish" conditions must be seen in light of actual biological history. These old prenatal exposures to powerful chemical compounds used in obstetric practice were very real and very acute, even if you did not ask or know about them.
SNORD115 regions were represented in 4 of the top 10 DMRs.Dani Fallin and Andrew Feinberg of John Hopkins University Center for Epigenetics, and colleagues, have found a DNA methylation pattern in the sperm of fathers with an increased risk of fathering autistic children that is also present in brains of unrelated autistic children. See the paper at the International Journal of Epidemiology, April 2015.
Looking at the sperm of fathers of young children considered at risk for autism, the team found 193 significant differentially methylated regions (DMRs), compared to controls; those sperm DMRs are large stretches of dozens of CpGs, not single CpG sites, and were consistent with 75 CpG probes from the 450K; and the DMRs are involved in developmental processes including imprinting disorders The aberrant methylation was associated with genomic areas involved in the imprinting disorders Angelman syndrome and Prader-Wili Syndrome. The region regulates neuron growth and produces important regulatory molecules. The large-scale methylation differences suggests epigenetic deviations in the germline may manifest as abnormalities in early brain development of offspring, producing the autism phenotype.  Three of the Hutchens children have idiopathic autism. Joan Hutchens and her husband have five children, and live in Silicon Valley. Joan shares her story: "Three of our five children are autistic, both of the boys and one of the three girls. Neither my husband or myself have any autism or developmental disabilities up our family trees, and my pregnancies were normal without any known risk factors. Why we would end up with three children with autism was a profound mystery to everyone. "I was born in Los Angeles in August 1965 at Cedars of Lebanon Hospital. Years ago, my mother told me that during her pregnancy with me her doctor had regularly injected her with drugs that he thought could help prevent miscarriage. My mother had a small frame and the pregnancy was considered 'at-risk' for that simple, if nutty, reason. "Though we could not locate my mom's 1964-65 medical records, based on the common medical practice at the time, those drugs were almost certainly synthetic steroid hormones, such as fake progesterones and estrogens, which were used prolifically in obstetrics of that era. "My friend Jill Escher, of the Escher Fund for Autism, and mom to two kids with equally mysterious autism, was born one month after me at the same Los Angeles hospital. Unlike me, though, she was successful in obtaining records of the multiple synthetic steroid drugs to which she was prenatally exposed. These drugs were very powerful, and operate by altering gene expression and function. "People always tell me that my kids' autism must be 'genetic,' since I have three of them, but how could that be when we have no history of this or related disorders in our families? I find it much more plausible that my prenatal drug exposures damaged my eggs, inducing scattershot 'de novo' alterations. "Given the enormous surge in autism cases, I don't understand why the germline disruption hypothesis is not the focal point for autism research today. We must stop analyzing so-called autism genes as if they have no exposure history." [Joan Hutchens is a pseudonym, used to protect her children's privacy. For any inquiries, she can be contacted through the Escher Fund for Autism.]  March 16, 2015 Re: Citizen Petition to Withdraw Approval for 17α-Hydroxyprogesterone Caproate (“17-OHPC,” Including Brand “Makena”) as a Drug Used in Pregnancy, Pending Fetal Germline Impact Assessment To the Commissioner of the Food and Drug Administration: The undersigned (or “Petitioner”) respectfully submits this petition in accordance with 21 C.F.R. 10.30 to request that the Commissioner of Food and Drugs withdraw approval for the drug 17-alpha hydroxyprogesterone caproate (“17-OHPC,” including brand “Makena”) as a drug used in pregnancy, pending assessment of potential deleterious impacts to the fetal germline. The undersigned was prenatally exposed to this drug in 1965, believes she has suffered injury as a result, and has located numerous similarly exposed individuals suffering similar unforeseen and grievous injury. The injuries are consistent with research demonstrating adverse epigenetic effects (“epimutation”) of hormone signal-disrupting compounds on the delicate process of fetal germline synthesis, with temporal associations between the introduction of the drug and the unexpected deleterious effects, and with mounting evidence that autism and related neurodevelopmental abnormalities are at least in part caused by de novo perturbations of the germline. The FDA may hesitate to re-evaluate a drug so long and so pervasively used. However, 17-OHPC was initially approved at a time before fetal germline vulnerability came to be broadly appreciated in biology and toxicology, and before generational effects of synthetic hormone signal disruption1 came to be appreciated. As when the thalidomide tragedy belatedly shattered the false belief in placental impermeability and shone a light on the particularly horrific nature of derangements occurring during critical developmental windows, and as when the diethylstilbestrol (DES) catastrophe upended conventional wisdom by revealing time-delayed or invisible effects of prenatal exposure, we now face a third wave of most unfortunate revelation: that pregnancy medications can, however inadvertently, “drug the DNA” of grandoffspring, a biological phenomenon that, once again, requires an urgent response by regulators.... Please read the entire Petition (PDF) here. 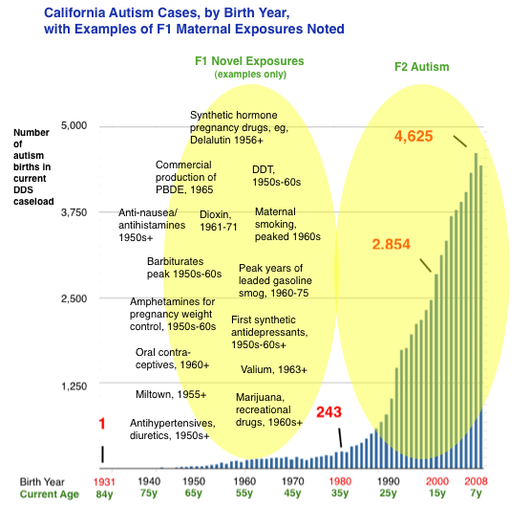
Clearly, many things contribute to the risk of the abnormal early neurodevelopment we label autism: genes (10%), prematurity/birth complications (probably 10%), assisted fertility, especially IVF (small amount), prenatal exposures to neurochemical-disruptive substances such as anticonvulsants and antidepressants (small amount), and more. But for the vast bulk of patients, etiology is unknown. Most research dollars focus on "gene hunting," with some funding going toward investigating proximal fetal exposures. But almost no money has been invested in how exposures have affected the integrity of our DNA. The vulnerable phase of fetal germline synthesis occurs approximately 20-40 years prior to conception, during the parents’ (F1) own fetal development. This dynamic phase involves specification and proliferation of germ cells, epigenetic reprogramming, and the laying of genomic imprints, among other phenomena. And in the 1950s, 60s, and 70s, these phenomena occurred in the context of many novel and toxic gestational exposures. Birth cohort data from California’s Department of Developmental Services (see above) indicate that autism births began a quasi exponential ascent starting in the early 1980s. This growth in DDS-eligible autism — a subset of autism involving more severe mental disability and functional limitations, and excluding the “high functioning” segment — has been repeatedly determined not attributable to diagnostic shift or broadening of eligibility criteria.1 California DDS autism numbered about 3,000 in the mid-1980s. Today the autism caseload exceeds 75,000. According to our hypothesis, a portion of this surge may result from developmental dysregulation resulting from molecular effects of old and largely forgotten exposures to the F1 parental germline. For developmental pathology in F2 offspring to have occurred in births in the 1980s and thereafter, germline errors would have occurred during the fetal development of the parental generation, in the 1950s and thereafter. Assuming induced germline errors are playing a role in the autism surge, the next logical question is what exposures increasingly affected the uterine environment in the 1950s, 60s, 70s, exposures that perhaps had been nonexistent or less common in prior decades, centuries, or even millennia? The answer could lie in many evolutionarily novel stressors. For example, maternal cigarette smoking became ubiquitous and peaked in the 1960s. In addition, a wide variety of novel substances were invented, marketed and used as pregnancy drugs, including synthetic “anti-miscarriage” hormones, anti-nausea drugs, painkillers, psychoactive drugs such as antidepressants and anti-anxiety medications, sleeping aids and sedatives, anesthesia, and more. Many of those drugs had powerful endocrine-disrupting or otherwise toxic effects. Medical radiation was applied to many pregnancies. Recreational drug use also surged in the 1960s. We hypothesize that many of these abnormal post-war in utero exposures to the parent generation (F1) could have acted as subtle fetal germline teratogens, inducing mutagenesis, epimutagenesis or both, resulting in dysregulation of development of the subsequent generation (F2). We further hypothesize that fetal germline exposures can result in heritability of autism or related neurodevelopmental disorders due to the likelihood of multiple gametes being affected by the same exposure. It would also result in heterogeneity because, in part, different gametes would be challenged in different ways by an exposure. It would also result in gender differences in offspring owing to epigenomic mechanisms that result in differential phenotypes according to gender, such as imprinting and X-chromosome inactivation. It would also result in demographic differences, since many of the exposures (for example, once-popular prophylactic synthetic hormone treatments) tended to be available to women of higher SES and located in metropolitan areas. Jill Escher fn1: See, for example, Autistic Spectrum Disorders, Changes in the California Caseload An Update: June 1987 – June 2007; and The Epidemiology of Autism in California (2002), noting “The observed increase in autism cases cannot be explained by a loosening in the criteria used to make the diagnosis,” and stating, “Has the increase in cases of autism been created artificially by having ‘missed’ the diagnosis in the past, and instead reporting autistic children as ‘mentally retarded?’ This explanation was not supported by our data.” Moreover, there is no signal or evidence that California’s singularly robust developmental services system has overlooked tens of thousands of mentally and developmentally disabled adults born prior to the 1980s (now over the age of 35) with the striking autism symptomology.  In April of 2013 I filed a Citizens Petition with the FDA in a first-stab attempt to wake the agency up about potential threat to fetal germline caused by pregnancy drugs. This particular petition involved a request that the FDA revoke its recently granted Class A approval of the morning sickness drug Diclegis, pending assessment of impact on fetal germline, and also revise pregnancy drug labeling to address risks to fetal germline.
You can find my petition linked above or in the FDA docket: http://www.regulations.gov/#!documentDetail;D=FDA-2013-P-0522-0001, or if that does not work, here: http://www.regulations.gov/#!docketDetail;D=FDA-2013-P-0522 In August of 2014, the FDA denied my petition. You can download that PDF or visit the docket: http://www.regulations.gov/#!documentDetail;D=FDA-2013-P-0522-0009 Why did I file this petition and what did the FDA say in response? I submitted the petition because the FDA continues to operate in a biologically bankrupt, factually incomplete, and outdated paradigm in how it assesses the risks of pregnancy drugs. And the consequences of its plodding "Let it become conventional wisdom, and then maybe we'll think about it" regulatory posture has spawned disastrous consequences. To the FDA, fetal germline simply does not exist, and to the extent there might be little critters in those cute little fetal gonads, they are unimportant and unworthy of protection. Imagine if the FDA told the public, "We will assess dangers of pregnancy drugs, but refuse to consider any effect on the heart. The heart is a difficult organ to study, so we just won't do it!" People would of course be dumbfounded at the flippant stupidity of such an attitude, and the staff would probably be fired in humiliation. But this is exactly what's happening at the FDA with regard to a different organ, the gonads, or at least the precious materials that lie within them. What did the FDA think about my petition? In response to my fairly non-controversial assertion that endocrine-disrupting and other chemicals can adversely affect mammalian germline, the FDA took the position that it was not their nor the manufacturer's burden to show safety, but rather it was my burden to prove the germline effects of Diclegis, or, presumably, any other drug that may enter a pregnant body. The agency, which doesn't even bother to ask the question about germline effects in its protocols, said that while I had offered support for the general proposition that hormonally active chemicals can impair germline synthesis, I had failed to offer "human or animal data for Diclegis which demonstrate or suggest that Diclegis disrupts the human fetal germ cell epigenome." My friend, a wise attorney, once offered me an analogy for this type of hyper-narrow regulatory approach. Imagine, she said, a red Ferrari drives down the highway at 100 miles per hour, crashes, and kills four people. Now, imagine that the lawmakers' response was to pass a bill preventing red Ferraris from hurtling down the highway at 100 mph. In this narrow approach, the hazards of other cars, perhaps moving at similar speeds, would be ignored. But this is the FDA's approach. A drug/chemical (by the way, there is no distinction between drugs and the broader category of chemicals except as to marketing and packaging, they are both just man-made molecules with biological effects) must have an exact molecular structure already proven harmful, otherwise it will bypass the artificially constrained regulatory apparatus. Next, the FDA actually admitted that no studies have yet examined germline or F2 effects of the drug, but was oddly unconcerned about that absence of information: "All of the articles address in utero and postnatal exposure in first generation (F1) offspring with a focus on congenital abnormalities/fetal malformation (for example, limb defects) and other birth defects (for example, clefts of lip and palate). None of the articles provides information on the second generation [F2 (grandchildren)]. DBRUP did not find any articles that demonstrated a risk to the fetal germline associated with the use of doxylamine and pyridoxine, alone or in combination, with resulting neurodevelopmental pathology in F2 offspring." Okay, let me get this straight. The FDA is basically saying, "We haven't bothered requiring F2 studies, so, um, that's somehow proof of lack of F2 impacts, or proof that F2 studies are not needed!" Okay, thanks FDA, that's very reassuring. Finally, the FDA in its vast wisdom stated that if no gross anatomical birth defects appear in F1, it sees absolutely no reason to be concerned about potential molecular impacts in the germline (F2). In other words, the agency has taken the position that it's impossible for the germline to be affected if there are no obvious somatic defects. Given that germ cells and somatic cells undergo completely different forms of molecular development and programming, I cannot figure out how the FDA reached that facile and falsely reassuring conclusion. In addition, the FDA is notorious for limiting its examination of somatic impacts to "birth defects" rather than long-term effects, including on neurodevelopment, or on subtle effects including sexual dimorphism of the brain, or personality effects, so its unwavering belief in the non-effects of Diclegis, based on studies that only surmised a portion of potential somatic cell effects, are surely premature. I also asked that the FDA recategorize Diclegis as a Category C drug instead of Category A, since no research has yet ascertained potential effects on fetal germline. Again, the FDA felt this question was unimportant, and eclipsed by the data showing no significant F1 somatic birth defects: "Given the extent of the human studies done to support the approval ofDiclegis (and Bendectin and Diclectin before that, as well as the clinical evidence that supports the OTC indications for doxylamine) that show no adverse effect on the fetus, we do not believe redesignation of Diclegis as Pregnancy Category C is appropriate." What does all this mean? Was my first stab at shaking the shoulders of the slumbering FDA a total failure? Should I try, try again? Here's my take on it (always subject to change). In some ways I think my petition was historic—it represented the first time in FDA history that anyone has raised the question about the potential adverse impacts of pregnancy drugs on fetal germline. Second, there is a growing appreciation among regulators and toxicologists concerning germline vulnerability, particularly during the fetal development phase, owing to the fine-tuned and evolutionarily conserved epigenetic reprogramming of the germ cells. So, perhaps in the next stab the general awareness of this phenomenon could make the regulators more open to these questions. And third, at a certain point, this humongous blind spot in how the FDA thinks about drug risk will just become plain obvious enough to everyone outside the FDA, that to save face the agency will need to finally address these questions head-on in the approval and labeling process. And right now, placing the burden on consumers to be PhDs in molecular biology with millions of dollars to fund private toxicological research in order to plead their case about a rather obvious question that should be inherent in the regulatory process, is just, well, pathetic and unconscionable. I do have a second petition planned, with regards to another popular pregnancy drug, and one with known endocrine-disrupting effects. It will raise urgent questions — questions that should by now be routine, but tragically are not. News on that coming soon. But the fundamental question is this: does the FDA exist, by Congressional mandate, to pro-actively protect human health, even somewhat ahead of the curve of conventional wisdom, or to defend its crusty old bureaucratic machinery stuck in convenient but biologically false bygone paradigms? At this point, it often appears to be the latter. This website aims to provide a central gathering point for information about germline epigenetics against the backdrop of environmental exposures. If this topic is of interest to you (and I hope it is!) I would like to point you to an earlier effort to put on the map the possible role of environmental epigenetics in autism.
The site, autismepigenetics.org, an archive of videos and other information from a March 2013 symposium on the topic sponsored by UC Davis MIND Institute, Autism Speaks and the Escher Fund for Autism. The outstanding speakers included: Jill Escher, autism parent and science philanthropist Amander Clark, Ph.D, UCLA, Department of Molecular Cell and Developmental Biology and Institute for Stem Cell Biology and Medicine. David Crews, Ph.D, Ashbel Smith Professor of Integrative Biology, and Psychology, University of Texas at Austin Dana Dolinoy, Ph.D, Searle Assistant Professor in Environmental Health Sciences, University of Michigan School of Public Health Dani Fallin, Ph.D, Johns Hopkins Bloomberg School of Public Health, professor of Epidemiology Andrea Gore, Ph.D, Gustavus & Louise Pfeiffer Professor of Pharmacology and Toxicology, University of Texas, Austin Alycia Halladay, Ph.D, Director of Research for Environmental Sciences, Autism Speaks. Janine LaSalle, Ph.D, Professor, UC Davis MIND Institute, studies the interplay of genetics, environmental factors, and epigenetics on human neurodevelopment and human health. Prof. Dr. Isabelle Mansuy, Brain Research Institute, University of Zurich Erik Lykke Mortensen, Cand. Psych, Professor, Department of Public Health, Copenhagen University Nancy Press, Ph.D, Professor, School of Nursing and Department of Public Health & Preventive Medicine, School of Medicine Emilie Rissman, Ph.D, Professor of Biochemistry & Molecular Genetics, University of Virginia Michael Skinner, Ph.D, Professor, Center for Reproductive Biology, School of Biological Sciences, Washington State University Adam Urato, MD, Tufts University School of Medicine, maternal-fetal medicine physician, assistant professor, Tufts University School of Medicine and chairman, Department of OB/GYN at MetroWest Medical Center in Framingham, Massachusetts Rosanna Weksberg, MD, Ph.D, Professor of Pediatrics and Molecular Genetics, Hospital for Children, Toronto Tracey Woodruff, Ph.D, MPH, Professor and Director, Program on Reproductive Health and the Environment, UCSF In Memory of Theo Colborn, who Cried Out for Understanding of the Menace of Hormone Disruption12/15/2014 by Jill Escher
I just heard that Theo Colborn, the great pioneer of endocrine disruption, and a true hero in my life, has passed away. Dr. Colborn understood the menacing ways hormone disruption can adulterate human development, and called on us as a society to explore this exquisite and vulnerable "inner space," instead of outer space, as in the video above. Thank you, Dr. Colborn, for working to protect the invisible world that makes us human. |
AuthorJill Escher, Escher Fund for Autism, is a California-based science philanthropist and mother of two children with severe autism, focused on the question of how environmentally induced germline disruptions may be contributing to today's epidemics of neurodevelopmental impairment. You can read about her discovery of her intensive prenatal exposure to synthetic hormone drugs here. Jill is also president of Autism Society San Francisco Bay Area. Archives
July 2021
Categories |

- Home
-
Expert Q&A
- Eva Jablonka Q&A
- Amander Clark Q&A
- Mirella Meyer-Ficca Q&A
- Janine LaSalle Q&A
- Dana Dolinoy Q&A
- Ben Laufer Q&A
- Tracy Bale Q&A
- Susan Murphy Q&A
- Alycia Halladay Q&A
- Wendy Chung Q&A
- Pradeep Bhide Q&A
- Pat Hunt Q&A
- Yauk and Marchetti Q&A
- Emilie Rissman Q&A
- Carol Kwiatkowski Q&A
- Linda Birnbaum Q&A
- Virender Rehan Q&A
- Carlos Guerrero-Bosagna Q&A
- Randy Jirtle Q&A
- Jerry Heindel Q&A
- Cheryl Walker Q&A
- Eileen McLaughlin Q&A
- Carmen Marsit Q&A
- Marisa Bartolomei Q&A
- Christopher Gregg Q&A
- Andrea Baccarelli Q&A
- David Moore Q&A
- Patrick Allard Q&A
- Catherine Dulac Q&A
- Lucas Argueso Q&A
- Toshi Shioda Q&A
- Miklos Toth Q&A
- Piroska Szabo Q&A
- Reinisch Q&A
- Klebanoff Q&A
- Denis Noble Q&A
- Germline in the News
- Science
- Presentations
- About Us
- Blog
 RSS Feed
RSS Feed
Proudly powered by Weebly